Do I Suffer From Overpronation
Overview
Over pronation of the foot is commonly referred to as "flat feet." Many middle-aged men and women suffer from over pronation over time and as a result of wearing poor-fitting shoes, continuing with repetitive exercising habits, or walking in high heels for long periods over several years. Regular speed-walkers often experience over pronation as well as a result of this activity.
Causes
You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation.
Symptoms
Over-Pronation may cause pain in the heel of the foot, the foot arch, under the ball of the foot, in the ankle, knee, hip or back. The symptoms may be localized to one particular area of the foot or may be experienced in any number of combinations. Standing for long periods of time, walking and running may become difficult due to the additional stress and/or discomfort accompanied with these activities. Upon Visual Inspection, when standing the heels of the foot lean inward and one or both of the knee caps may turn inward.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Prevention
Many of the prevention methods for overpronation-orthotics, for example-can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function.
Over pronation of the foot is commonly referred to as "flat feet." Many middle-aged men and women suffer from over pronation over time and as a result of wearing poor-fitting shoes, continuing with repetitive exercising habits, or walking in high heels for long periods over several years. Regular speed-walkers often experience over pronation as well as a result of this activity.
Causes
You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation.
Symptoms
Over-Pronation may cause pain in the heel of the foot, the foot arch, under the ball of the foot, in the ankle, knee, hip or back. The symptoms may be localized to one particular area of the foot or may be experienced in any number of combinations. Standing for long periods of time, walking and running may become difficult due to the additional stress and/or discomfort accompanied with these activities. Upon Visual Inspection, when standing the heels of the foot lean inward and one or both of the knee caps may turn inward.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Prevention
Many of the prevention methods for overpronation-orthotics, for example-can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function.
Rehab And Severs Disease
Overview
Sever?s disease is an inflammation of the growth plate in the heel, which is an area at the end of the developing bone where cartilage gradually turns into bone as kids grow. In fact, kids grow so rapidly at this age that their muscles and tendons can?t quite keep up with their feet and legs. This leaves the muscles and tendons tight and overstretched, particularly the Achilles tendon that connects the heel to the calf muscles. In fast-growing preteen and teen athletes, it can put so much pressure on the heel?s growth plate that it swells and becomes tender.
Causes
The usual cause is directly related to overuse of the bone and tendons in the heel. This can come from playing sports or anything that involves a lot of heel movement. It can be associated with starting a new sport, or the start of a new season, or too much weight bearing on the heel. Also, excessive traction could cause this, since the bones and tendons are still developing. Many children who over pronate their feet exhibit symptoms and in most patients, it usually involves both heels.
Symptoms
Children aged between 8 to 13 years of age can experience Sever?s disease with girls being normally younger and boys slightly older. Sever?s disease normally involves the back of the heel bone becoming painful towards the end of intense or prolonged activity and can remain painful after the activity for a few hours. Severe cases can result in limping and pain that can even remain the next morning after sport.
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot.
Non Surgical Treatment
There is nothing you can do to stop severs disease. It will stop when you finish growing. However the following will help to relieve the symptoms. Rest. Cut down on the time you spend playing sport until the pain has gone. Avoid sports that involve a lot of running or jumping. Swimming can be a useful alternative. Ice the affected area for ten to 15 minutes, especially after activity. Make sure you protect the skin by wrapping the ice in a towel. Elevate (raise) the leg when painful and swollen especially after sports. Pain relieving medication may reduce pain and swelling, but you need to discuss options with a pharmacist or GP. Always wear shoes. Avoid activities in bare feet. Choose a supportive shoe with the laces done up.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Sever?s disease is an inflammation of the growth plate in the heel, which is an area at the end of the developing bone where cartilage gradually turns into bone as kids grow. In fact, kids grow so rapidly at this age that their muscles and tendons can?t quite keep up with their feet and legs. This leaves the muscles and tendons tight and overstretched, particularly the Achilles tendon that connects the heel to the calf muscles. In fast-growing preteen and teen athletes, it can put so much pressure on the heel?s growth plate that it swells and becomes tender.
Causes
The usual cause is directly related to overuse of the bone and tendons in the heel. This can come from playing sports or anything that involves a lot of heel movement. It can be associated with starting a new sport, or the start of a new season, or too much weight bearing on the heel. Also, excessive traction could cause this, since the bones and tendons are still developing. Many children who over pronate their feet exhibit symptoms and in most patients, it usually involves both heels.
Symptoms
Children aged between 8 to 13 years of age can experience Sever?s disease with girls being normally younger and boys slightly older. Sever?s disease normally involves the back of the heel bone becoming painful towards the end of intense or prolonged activity and can remain painful after the activity for a few hours. Severe cases can result in limping and pain that can even remain the next morning after sport.
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot.
Non Surgical Treatment
There is nothing you can do to stop severs disease. It will stop when you finish growing. However the following will help to relieve the symptoms. Rest. Cut down on the time you spend playing sport until the pain has gone. Avoid sports that involve a lot of running or jumping. Swimming can be a useful alternative. Ice the affected area for ten to 15 minutes, especially after activity. Make sure you protect the skin by wrapping the ice in a towel. Elevate (raise) the leg when painful and swollen especially after sports. Pain relieving medication may reduce pain and swelling, but you need to discuss options with a pharmacist or GP. Always wear shoes. Avoid activities in bare feet. Choose a supportive shoe with the laces done up.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
What Exactly Is Posterior Tibial Tendon Dysfunction ?
Overview
Dysfunction of the tibialis posterior tendon is a common condition and a common cause of acquired flatfoot deformity in adults. Women older than 40 are most at risk. Patients present with pain and swelling of the medial hindfoot. Patients may also report a change in the shape of the foot or flattening of the foot. The foot develops a valgus heel (the heel rotates laterally when observed from behind), a flattened longitudinal arch, and an abducted forefoot. Conservative treatment includes non-steroidal anti-inflammatory drugs, rest, and immobilisation for acute inflammation; and orthoses to control the more chronic symptoms. Surgical treatment in the early stages is hindfoot osteotomy combined with tendon transfer. Arthrodesis of the hindfoot, and occasionally the ankle, is required in the surgical treatment of the later stages of tibialis posterior dysfunction. 
Causes
Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs.
Symptoms
In many cases, adult flatfoot causes no pain or problems. In others, pain may be severe. Many people experience aching pain in the heel and arch and swelling along the inner side of the foot.
Diagnosis
In diagnosing flatfoot, the foot & Ankle surgeon examines the foot and observes how it looks when you stand and sit. Weight bearing x-rays are used to determine the severity of the disorder. Advanced imaging, such as magnetic resonance imaging (MRI) and computed tomography (CAT or CT) scans may be used to assess different ligaments, tendons and joint/cartilage damage. The foot & Ankle Institute has three extremity MRI?s on site at our Des Plaines, Highland Park, and Lincoln Park locations. These extremity MRI?s only take about 30 minutes for the study and only requires the patient put their foot into a painless machine avoiding the uncomfortable Claustrophobia that some MRI devices create.
Non surgical Treatment
Medical or nonoperative therapy for posterior tibial tendon dysfunction involves rest, immobilization, nonsteroidal anti-inflammatory medication, physical therapy, orthotics, and bracing. This treatment is especially attractive for patients who are elderly, who place low demands on the tendon, and who may have underlying medical problems that preclude operative intervention. During stage 1 posterior tibial tendon dysfunction, pain, rather than deformity, predominates. Cast immobilization is indicated for acute tenosynovitis of the posterior tibial tendon or for patients whose main presenting feature is chronic pain along the tendon sheath. A well-molded short leg walking cast or removable cast boot should be used for 6-8 weeks. Weight bearing is permitted if the patient is able to ambulate without pain. If improvement is noted, the patient then may be placed in custom full-length semirigid orthotics. The patient may then be referred to physical therapy for stretching of the Achilles tendon and strengthening of the posterior tibial tendon. Steroid injection into the posterior tibial tendon sheath is not recommended due to the possibility of causing a tendon rupture. In stage 2 dysfunction, a painful flexible deformity develops, and more control of hindfoot motion is required. In these cases, a rigid University of California at Berkley (UCBL) orthosis or short articulated ankle-foot orthosis (AFO) is indicated. Once a rigid flatfoot deformity develops, as in stage 3 or 4, bracing is extended above the ankle with a molded AFO, double upright brace, or patellar-tendon-bearing brace. The goals of this treatment are to accommodate the deformity, prevent or slow further collapse, and improve walking ability by transferring load to the proximal leg away from the collapsed medial midfoot and heel. 
Surgical Treatment
For more chronic flatfoot pain, surgical intervention may be the best option. Barring other serious medical ailments, surgery is a good alternative for patients with a serious problem. There are two surgical options depending on a person?s physical condition, age and lifestyle. The first type of surgery involves repair of the PTT by transferring of a nearby tendon to help re-establish an arch and straighten out the foot. After this surgery, patients wear a non-weight bearing support boot for four to six weeks. The other surgery involves fusing of two or three bones in the hind foot below the ankle. While providing significant pain relief, this option does take away some hind foot side-to-side motion. Following surgery, patients are in a cast for three months. Surgery is an effective treatment to address adult-acquired flatfoot, but it can sometimes be avoided if foot issues are resolved early. That is why it is so important to seek help right away if you are feeling ankle pain. But perhaps the best way to keep from becoming flatfooted is to avoid the risk factors altogether. This means keeping your blood pressure, weight and diabetes in check.
Understand Heel Discomfort
Overview
Every mile you walk puts tons of stress on each foot. Your feet can handle a heavy load, but too much stress pushes them over their limits. When you pound your feet on hard surfaces playing sports or wear shoes that irritate sensitive tissues, you may develop heel pain, the most common problem affecting the foot and ankle. A sore heel will usually get better on its own without surgery if you give it enough rest. However, many people ignore the early signs of Heel Pain and keep on doing the activities that caused it. When you continue to walk on a sore heel, it will only get worse and could become a chronic condition leading to more problems.
Causes
Plantar Fasciitis is the most common form of heel pain. The tears and inflammation that develop along the plantar fascia ligament result in dull aching pain or a burning sensation along the bottom of the foot. Pain becomes particularly noticeable after periods of rest, such as during the first few steps after getting out of bed in the morning, or after getting up after a prolonged period of sitting. Another common form of heel pain is the development of a heel spur. A heel spur, as mentioned above, is the formation of a bony hook extending from the heel. Typically, these growths develop near the area where the plantar fascia connects to the heel bone. The repetitive pressure on the plantar fascia that results from stretching excessively away from the heel bone causes a response from our body that delivers calcium to the area. The heel pain that ensues develops from the nerves and sensitive tissue that become irritated when the bone fragment digs into the bottom of the heel. Pain may decrease after walking as the tissue in the heel gets used to the fragment and adjusts around it. However, pain will be particularly problematic following periods of rest. Strained muscle tissue may cause heel pain in several areas. A tight plantar fascia causes additional tension, particularly while exercising, placing runners and other athletes at risk if the ligament is not properly warmed up prior to exercise. Additionally, a tight Achilles tendon along the back of the foot can also add tension along the plantar fascia, resulting in possible damage, not to mention the damage and pain that can occur along the Achilles tendon itself (Achilles tendonitis). It is recommended that athletes properly stretch the foot as well as the calf in order to reduce tension on muscle and other tissue in the foot.
Symptoms
Initially, this pain may only be present when first standing up after sleeping or sitting. As you walk around, the muscle and tendon loosen and the pain goes away. As this problem progresses, the pain can be present with all standing and walking. You may notice a knot or bump on the back of the heel. Swelling may develop. In some cases, pressure from the back of the shoe causes pain.
Diagnosis
A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem.
Non Surgical Treatment
Treatments to add to your stretching program include wearing good-quality shoes, icing the painful area, and massaging the arch. Do not walk barefoot; walk in shoes with good heel and arch supports such as high-quality walking or running shoes. Keep a pair of shoes next to your bed so you can put them on before taking your first step. Your doctor may recommend that you wear an additional arch support or a heel cup in the shoes. Icing your foot can help relieve pain. Rub a frozen bottle of water or an ice cup over the tender areas for five minutes two times each day. Massage your foot by rolling a tennis, golf ball, or baseball along your sole and heel. This friction massage can help break up adhesions and stretch the plantar fascia. Do this for five minutes two times each day. If you are a runner or just started a walking or running program, evaluate your training for errors such as warming up improperly, increasing mileage too quickly, running hills excessively, running on surfaces that are too hard, or wearing broken down shoes. Adjusting your training program can help relieve your pain. While recovering from heel pain, walk or jog in a pool or crosstrain by biking and swimming. These activities maintain your cardiovascular fitness without stressing your heel cord or plantar fascia. Heel pain takes time to go away. Be patient and remember that no treatment is a substitute for STRETCHING!
Surgical Treatment
Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
Prevention

Wear properly fitting shoes. Place insoles or inserts in your shoes to help control abnormal foot motion. Maintain a healthy weight. Exercise and do foot stretches as they have been shown to decrease the incidence of heel pain.
Every mile you walk puts tons of stress on each foot. Your feet can handle a heavy load, but too much stress pushes them over their limits. When you pound your feet on hard surfaces playing sports or wear shoes that irritate sensitive tissues, you may develop heel pain, the most common problem affecting the foot and ankle. A sore heel will usually get better on its own without surgery if you give it enough rest. However, many people ignore the early signs of Heel Pain and keep on doing the activities that caused it. When you continue to walk on a sore heel, it will only get worse and could become a chronic condition leading to more problems.
Causes
Plantar Fasciitis is the most common form of heel pain. The tears and inflammation that develop along the plantar fascia ligament result in dull aching pain or a burning sensation along the bottom of the foot. Pain becomes particularly noticeable after periods of rest, such as during the first few steps after getting out of bed in the morning, or after getting up after a prolonged period of sitting. Another common form of heel pain is the development of a heel spur. A heel spur, as mentioned above, is the formation of a bony hook extending from the heel. Typically, these growths develop near the area where the plantar fascia connects to the heel bone. The repetitive pressure on the plantar fascia that results from stretching excessively away from the heel bone causes a response from our body that delivers calcium to the area. The heel pain that ensues develops from the nerves and sensitive tissue that become irritated when the bone fragment digs into the bottom of the heel. Pain may decrease after walking as the tissue in the heel gets used to the fragment and adjusts around it. However, pain will be particularly problematic following periods of rest. Strained muscle tissue may cause heel pain in several areas. A tight plantar fascia causes additional tension, particularly while exercising, placing runners and other athletes at risk if the ligament is not properly warmed up prior to exercise. Additionally, a tight Achilles tendon along the back of the foot can also add tension along the plantar fascia, resulting in possible damage, not to mention the damage and pain that can occur along the Achilles tendon itself (Achilles tendonitis). It is recommended that athletes properly stretch the foot as well as the calf in order to reduce tension on muscle and other tissue in the foot.
Symptoms
Initially, this pain may only be present when first standing up after sleeping or sitting. As you walk around, the muscle and tendon loosen and the pain goes away. As this problem progresses, the pain can be present with all standing and walking. You may notice a knot or bump on the back of the heel. Swelling may develop. In some cases, pressure from the back of the shoe causes pain.
Diagnosis
A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem.
Non Surgical Treatment
Treatments to add to your stretching program include wearing good-quality shoes, icing the painful area, and massaging the arch. Do not walk barefoot; walk in shoes with good heel and arch supports such as high-quality walking or running shoes. Keep a pair of shoes next to your bed so you can put them on before taking your first step. Your doctor may recommend that you wear an additional arch support or a heel cup in the shoes. Icing your foot can help relieve pain. Rub a frozen bottle of water or an ice cup over the tender areas for five minutes two times each day. Massage your foot by rolling a tennis, golf ball, or baseball along your sole and heel. This friction massage can help break up adhesions and stretch the plantar fascia. Do this for five minutes two times each day. If you are a runner or just started a walking or running program, evaluate your training for errors such as warming up improperly, increasing mileage too quickly, running hills excessively, running on surfaces that are too hard, or wearing broken down shoes. Adjusting your training program can help relieve your pain. While recovering from heel pain, walk or jog in a pool or crosstrain by biking and swimming. These activities maintain your cardiovascular fitness without stressing your heel cord or plantar fascia. Heel pain takes time to go away. Be patient and remember that no treatment is a substitute for STRETCHING!
Surgical Treatment
Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
Prevention
Wear properly fitting shoes. Place insoles or inserts in your shoes to help control abnormal foot motion. Maintain a healthy weight. Exercise and do foot stretches as they have been shown to decrease the incidence of heel pain.
What Should I Do About Achilles Tendinitis ?
Overview
 Achilles tendonitis is inflammation of the tendon, usually resulting from overuse associated with a change in playing surface, footwear or intensity of an activity. The Achilles tendon is surrounded by a connective tissue sheath (paratenon, or 'paratendon'), rather than a true synovial sheath. The paratenon stretches with movement, allowing maximum gliding action. Near the insertion of the tendon are two bursae - the subcutaneous calcaneal and the retrocalcaneal bursae.
Achilles tendonitis is inflammation of the tendon, usually resulting from overuse associated with a change in playing surface, footwear or intensity of an activity. The Achilles tendon is surrounded by a connective tissue sheath (paratenon, or 'paratendon'), rather than a true synovial sheath. The paratenon stretches with movement, allowing maximum gliding action. Near the insertion of the tendon are two bursae - the subcutaneous calcaneal and the retrocalcaneal bursae.
Causes
When you place a large amount of stress on your Achilles tendon too quickly, it can become inflamed from tiny tears that occur during the activity. Achilles tendonitis is often a result of overtraining, or doing too much too soon. Excessive hill running can contribute to it. Flattening of the arch of your foot can place you at increased risk of developing Achilles tendonitis because of the extra stress placed on your Achilles tendon when walking or running.
Symptoms
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
When diagnosing Achilles tendinitis, a doctor will ask the patient a few questions about their symptoms and then perform a physical examination. To perform a physical exam on the Achilles tendon, the doctor will lightly touch around the back of the ankle and tendon to locate the source of the pain or inflammation. They will also test the foot and ankle to see if their range of motion and flexibility has been impaired. The doctor might also order an imaging test to be done on the tendon. This will aid in the elimination of other possible causes of pain and swelling, and may help the doctor assess the level of damage (if any) that has been done to the tendon. Types of imaging tests that could be used for diagnosing Achilles tendinitis are MRI (Magnetic resonance imaging), X-ray, Ultrasound.
Nonsurgical Treatment
Most cases of Achilles tendonitis can be treated at home. Here's what to do. Stop doing the activity that led to the injury. Avoid putting stress on your legs and feet, and give your tendon plenty of time to fully recover. Use the RICE formula. Don't exercise for a few days, or try an exercise that doesn't stress your feet, such as swimming. If necessary, your doctor may recommend that you use crutches or wear a walking boot to keep weight off your foot. Apply an ice pack wrapped in a towel or a cold compress to your tendon for 15 minutes or more after you exercise or if you feel pain in the tendon. Use tape or an athletic wrap to keep swelling down and help support and immobilize the tendon. Lie down and raise your foot above the level of your heart, and if possible, try to sleep with your foot elevated. This will help keep the swelling to a minimum. Take anti-inflammatory medications. Pain relievers like ibuprofen can help ease pain and reduce swelling in the affected area. Stretch and exercise your ankles and calf muscles while you recover. Keeping your muscles, tendons, and ligaments strong and flexible will aid in your recovery and help you keep from reinjuring your Achilles tendon. A doctor or a physical therapist can help you come up with a good exercise program. Try a pair of prescription orthotic inserts for your shoes if your doctor thinks it will help. Sometimes orthotics can be helpful. Talk to your doctor or someone trained in fitting orthotics to find out if they might work for you. Achilles tendon surgery is rarely needed. It's usually only done if the tendon breaks, and then only as a last resort after other methods of therapy have been tried. Most cases of Achilles tendonitis will get better on their own with rest and minor treatment.

Surgical Treatment
Surgery can be done to remove hardened fibrous tissue and repair any small tendon tears as a result of repetitive use injuries. This approach can also be used to help prevent an Achilles tendon rupture. If your Achilles tendon has already ruptured or torn, Achilles tendon surgery can be used to reattach the ends of the torn tendon. This approach is more thorough and definitive compared to non surgical treatment options discussed above. Surgical reattachment of the tendon also minimizes the change of re-rupturing the Achilles tendon.
Prevention
Suggestions to reduce your risk of Achilles tendonitis include, incorporate stretching into your warm-up and cool-down routines, maintain an adequate level of fitness for your sport, avoid dramatic increases in sports training, if you experience pain in your Achilles tendon, rest the area. Trying to ?work through? the pain will only make your injury worse, wear good quality supportive shoes appropriate to your sport. If there is foot deformity or flattening, obtain orthoses, avoid wearing high heels on a regular basis. Maintaining your foot in a ?tiptoe? position shortens your calf muscles and reduces the flexibility of your Achilles tendon. An inflexible Achilles tendon is more susceptible to injury, maintain a normal healthy weight.
Achilles tendonitis is inflammation of the tendon, usually resulting from overuse associated with a change in playing surface, footwear or intensity of an activity. The Achilles tendon is surrounded by a connective tissue sheath (paratenon, or 'paratendon'), rather than a true synovial sheath. The paratenon stretches with movement, allowing maximum gliding action. Near the insertion of the tendon are two bursae - the subcutaneous calcaneal and the retrocalcaneal bursae.
Causes
When you place a large amount of stress on your Achilles tendon too quickly, it can become inflamed from tiny tears that occur during the activity. Achilles tendonitis is often a result of overtraining, or doing too much too soon. Excessive hill running can contribute to it. Flattening of the arch of your foot can place you at increased risk of developing Achilles tendonitis because of the extra stress placed on your Achilles tendon when walking or running.
Symptoms
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
When diagnosing Achilles tendinitis, a doctor will ask the patient a few questions about their symptoms and then perform a physical examination. To perform a physical exam on the Achilles tendon, the doctor will lightly touch around the back of the ankle and tendon to locate the source of the pain or inflammation. They will also test the foot and ankle to see if their range of motion and flexibility has been impaired. The doctor might also order an imaging test to be done on the tendon. This will aid in the elimination of other possible causes of pain and swelling, and may help the doctor assess the level of damage (if any) that has been done to the tendon. Types of imaging tests that could be used for diagnosing Achilles tendinitis are MRI (Magnetic resonance imaging), X-ray, Ultrasound.
Nonsurgical Treatment
Most cases of Achilles tendonitis can be treated at home. Here's what to do. Stop doing the activity that led to the injury. Avoid putting stress on your legs and feet, and give your tendon plenty of time to fully recover. Use the RICE formula. Don't exercise for a few days, or try an exercise that doesn't stress your feet, such as swimming. If necessary, your doctor may recommend that you use crutches or wear a walking boot to keep weight off your foot. Apply an ice pack wrapped in a towel or a cold compress to your tendon for 15 minutes or more after you exercise or if you feel pain in the tendon. Use tape or an athletic wrap to keep swelling down and help support and immobilize the tendon. Lie down and raise your foot above the level of your heart, and if possible, try to sleep with your foot elevated. This will help keep the swelling to a minimum. Take anti-inflammatory medications. Pain relievers like ibuprofen can help ease pain and reduce swelling in the affected area. Stretch and exercise your ankles and calf muscles while you recover. Keeping your muscles, tendons, and ligaments strong and flexible will aid in your recovery and help you keep from reinjuring your Achilles tendon. A doctor or a physical therapist can help you come up with a good exercise program. Try a pair of prescription orthotic inserts for your shoes if your doctor thinks it will help. Sometimes orthotics can be helpful. Talk to your doctor or someone trained in fitting orthotics to find out if they might work for you. Achilles tendon surgery is rarely needed. It's usually only done if the tendon breaks, and then only as a last resort after other methods of therapy have been tried. Most cases of Achilles tendonitis will get better on their own with rest and minor treatment.
Surgical Treatment
Surgery can be done to remove hardened fibrous tissue and repair any small tendon tears as a result of repetitive use injuries. This approach can also be used to help prevent an Achilles tendon rupture. If your Achilles tendon has already ruptured or torn, Achilles tendon surgery can be used to reattach the ends of the torn tendon. This approach is more thorough and definitive compared to non surgical treatment options discussed above. Surgical reattachment of the tendon also minimizes the change of re-rupturing the Achilles tendon.
Prevention
Suggestions to reduce your risk of Achilles tendonitis include, incorporate stretching into your warm-up and cool-down routines, maintain an adequate level of fitness for your sport, avoid dramatic increases in sports training, if you experience pain in your Achilles tendon, rest the area. Trying to ?work through? the pain will only make your injury worse, wear good quality supportive shoes appropriate to your sport. If there is foot deformity or flattening, obtain orthoses, avoid wearing high heels on a regular basis. Maintaining your foot in a ?tiptoe? position shortens your calf muscles and reduces the flexibility of your Achilles tendon. An inflexible Achilles tendon is more susceptible to injury, maintain a normal healthy weight.
What Exactly Leads To Plantar Fasciitis
Overview
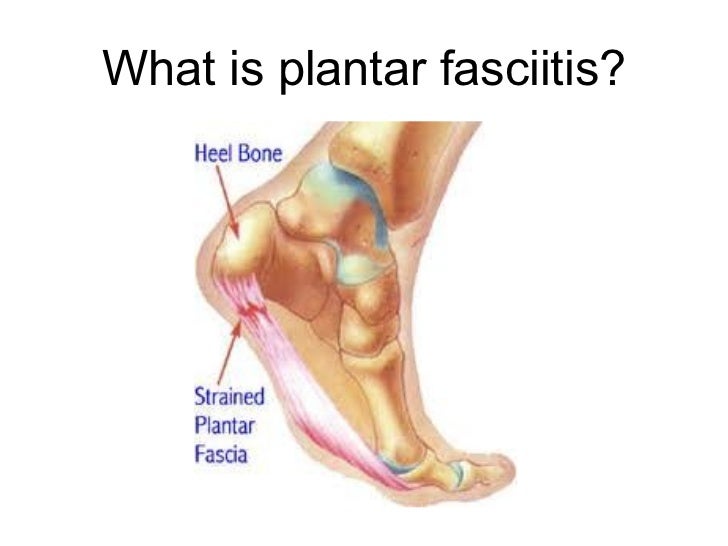
The plantar fascia is a thickened fibrous aponeurosis that originates from the medial tubercle of the calcaneus, runs forward to insert into the deep, short transverse ligaments of the metatarsal heads, dividing into 5 digital bands at the metatarsophalangeal joints and continuing forward to form the fibrous flexor sheathes on the plantar aspect of the toes. Small plantar nerves are invested in and around the plantar fascia, acting to register and mediate pain.
Causes
Repeated small injuries to the fascia (with or without inflammation) are thought to be the cause of plantar fasciitis. The injury is usually near to where the plantar fascia attaches to your heel bone. You are more likely to injure your plantar fascia in certain situations. For example, if you are on your feet for a lot of the time, or if you do lots of walking, running, standing, etc, when you are not used to it. (Plantar fasciitis may be confused with 'Policeman's heel', but they are different. Policeman's heel is plantar calcaneal bursitis - inflammation of the sack of fluid (bursa) under the heel bone. This is not as common as plantar fasciitis.) Also, people with a sedentary lifestyle are more prone to plantar fasciitis. If you have recently started exercising on a different surface, for example, running on the road instead of a track. If you have been wearing shoes with poor cushioning or poor arch support. If you are overweight this will put extra strain on your heel. If there is overuse or sudden stretching of your sole. For example, athletes who increase running intensity or distance; poor technique starting 'off the blocks', etc. If you have a tight Achilles tendon (the big tendon at the bottom of your calf muscles above your heel). This can affect your ability to flex your ankle and make you more likely to damage your plantar fascia. Often there is no apparent cause for plantar fasciitis, particularly in older people. A common wrong belief is that the pain is due to a bony growth or 'spur' coming from the heel bone (calcaneum). Many people have a bony spur of the heel bone but not everyone with this gets plantar fasciitis.
Symptoms
Symptoms of plantar fasciitis can occur suddenly or gradually. When they occur suddenly, there is usually intense heel pain on taking the first morning steps, known as first-step pain. This heel pain will often subside as you begin to walk around, but it may return in the late afternoon or evening. When symptoms occur gradually, a more long-lasting form of heel pain will cause you to shorten your stride while running or walking. You also may shift your weight toward the front of the foot, away from the heel.
Diagnosis
After you describe your symptoms and discuss your concerns, your doctor will examine your foot. Your doctor will look for these signs. A high arch, an area of maximum tenderness on the bottom of your foot, just in front of your heel bone. Pain that gets worse when you flex your foot and the doctor pushes on the plantar fascia. The pain improves when you point your toes down. Limited "up" motion of your ankle. Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods.
Non Surgical Treatment
You may experience concern in reading about treatment options for this condition that involve taking medications, having injections or undergoing surgery. While these remedies may be necessary in some cases, there are natural, non-invasive, affordable methods for treating and healing Plantar Fasciitis. A simple, three-step approach may be all you need to experience immediate or rapid symptom relief. Step 1) Give Your Feet A Rest. When a ligament is stressed and inflamed, it is absolutely essential to take pressure off it and let it rest. Adjust your daily habits to spend some time each day off your feet. Step 2) Ice Brings Cooling Relief. Apply an ice bag or cold pack to your heel for twenty minutes, twice a day. This will numb soreness and help control inflammation. Step 3) Gain Support From Orthotics. Orthotics are devices designed to modify body motions or lessen pressure on areas of the body. In the case of foot orthotics, these products may include splints, wraps and shoe inserts.
Surgical Treatment
Most practitioners agree that treatment for plantar fasciitis is a slow process. Most cases resolve within a year. If these more conservative measures don't provide relief after this time, your doctor may suggest other treatment. In such cases, or if your heel pain is truly debilitating and interfering with normal activity, your doctor may discuss surgical options with you. The most common surgery for plantar fasciitis is called a plantar fascia release and involves releasing a portion of the plantar fascia from the heel bone. A plantar fascia release can be performed through a regular incision or as endoscopic surgery, where a tiny incision allows a miniature scope to be inserted and surgery to be performed. About one in 20 patients with plantar fasciitis will need surgery. As with any surgery, there is still some chance that you will continue to have pain afterwards.
Prevention
Being overweight can place excess pressure and strain on your feet, particularly on your heels. Losing weight, and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet, can be beneficial for your feet. Wearing appropriate footwear is also important. Ideally, you should wear shoes with a low to moderate heel that supports and cushions your arches and heels. Avoid wearing shoes with no heels.
What Can Cause Plantar Fasciitis To Surface

Overview
Plantar fasciitis causes pain in the bottom of the heel. The plantar fascia is a thin ligament that connects your heel to the front of your foot. It supports the arch in your foot and is important in helping you walk. Plantar fasciitis is one of the most common orthopedic complaints. Your plantar fascia ligaments experience a lot of wear and tear in your daily life. Normally, these ligaments act as shock absorbers, supporting the arch of the foot. Too much pressure on your feet can damage or tear the ligaments. The plantar fascia becomes inflamed, and the inflammation causes heel pain and stiffness.
Causes
Inappropriate footwear is the No. 1 cause of plantar fasciosis. Footwear that possesses toe spring and a tapered toe box holds your big toe in an adducted and extended position. In this position, your abductor hallucis muscle-the muscle responsible for moving your big toe away from your foot’s midline-pulls on a foot structure called the flexor retinaculum and may restrict blood flow through your posterior tibial artery, the vessel that carries blood to the bottom of your foot. Tissues in the sole of your feet begin to degenerate as blood supply to this area is decreased. Other recognized causes of or contributors to this health problem include the following, calf muscle shortening, plantar fascia contracture, Obesity, rheumatoid arthritis, reactive arthritis, Psoriatic arthritis, Corticosteroid injections.
Symptoms
Among the symptoms for Plantar Fasciitis is pain usually felt on the underside of the heel, often most intense with the first steps after getting out of bed in the morning. It is commonly associated with long periods of weight bearing or sudden changes in weight bearing or activity. Plantar Fasciitis also called “policeman’s heel” is presented by a sharp stabbing pain at the bottom or front of the heel bone. In most cases, heel pain is more severe following periods of inactivity when getting up and then subsides, turning into a dull ache.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
The good news is that plantar fasciitis is reversible and very successfully treated. About 90 percent of people with plantar fasciitis improve significantly within two months of initial treatment. If your plantar fasciitis continues after a few months of conservative treatment, your doctor may inject your heel with steroidal anti-inflammatory medications (corticosteroid). Cortisone injections have been shown to have short-term benefits but they actually retard your progress in the medium to long-term, which usually means that you will suffer recurrent bouts for longer. Due to poor foot biomechanics being the primary cause of your plantar fasciitis it is vital to thoroughly assess and correct your foot and leg biomechanics to prevent future plantar fasciitis episodes or the development of a heel spur. Your physiotherapist is an expert in foot assessment and its dynamic biomechanical correction. They may recommend that you seek the advice of a podiatrist, who is an expert in the prescription on passive foot devices such as orthotics.

Surgical Treatment
Most patients have good results from surgery. However, because surgery can result in chronic pain and dissatisfaction, it is recommended only after all nonsurgical measures have been exhausted. The most common complications of release surgery include incomplete relief of pain and nerve damage.
Stretching Exercises
You may begin exercising the muscles of your foot right away by gently stretching them as follows. Prone hip extension, Lie on your stomach with your legs straight out behind you. Tighten up your buttocks muscles and lift one leg off the floor about 8 inches. Keep your knee straight. Hold for 5 seconds. Then lower your leg and relax. Do 3 sets of 10. Towel stretch, Sit on a hard surface with one leg stretched out in front of you. Loop a towel around your toes and the ball of your foot and pull the towel toward your body keeping your knee straight. Hold this position for 15 to 30 seconds then relax. Repeat 3 times. When the towel stretch becomes too easy, you may begin doing the standing calf stretch. Standing calf stretch, Facing a wall, put your hands against the wall at about eye level. Keep one leg back with the heel on the floor, and the other leg forward. Turn your back foot slightly inward (as if you were pigeon-toed) as you slowly lean into the wall until you feel a stretch in the back of your calf. Hold for 15 to 30 seconds. Repeat 3 times. Do this exercise several times each day. Sitting plantar fascia stretch, Sit in a chair and cross one foot over your other knee. Grab the base of your toes and pull them back toward your leg until you feel a comfortable stretch. Hold 15 seconds and repeat 3 times. When you can stand comfortably on your injured foot, you can begin standing to stretch the bottom of your foot using the plantar fascia stretch. Achilles stretch, Stand with the ball of one foot on a stair. Reach for the bottom step with your heel until you feel a stretch in the arch of your foot. Hold this position for 15 to 30 seconds and then relax. Repeat 3 times. After you have stretched the bottom muscles of your foot, you can begin strengthening the top muscles of your foot. Frozen can roll, Roll your bare injured foot back and forth from your heel to your mid-arch over a frozen juice can. Repeat for 3 to 5 minutes. This exercise is particularly helpful if done first thing in the morning. Towel pickup, With your heel on the ground, pick up a towel with your toes. Release. Repeat 10 to 20 times. When this gets easy, add more resistance by placing a book or small weight on the towel. Balance and reach exercises, Stand upright next to a chair. This will provide you with balance if needed. Stand on the foot farthest from the chair. Try to raise the arch of your foot while keeping your toes on the floor. Keep your foot in this position and reach forward in front of you with your hand farthest away from the chair, allowing your knee to bend. Repeat this 10 times while maintaining the arch height. This exercise can be made more difficult by reaching farther in front of you. Do 2 sets. Stand in the same position as above. While maintaining your arch height, reach the hand farthest away from the chair across your body toward the chair. The farther you reach, the more challenging the exercise. Do 2 sets of 10. Heel raise, Balance yourself while standing behind a chair or counter. Using the chair to help you, raise your body up onto your toes and hold for 5 seconds. Then slowly lower yourself down without holding onto the chair. Hold onto the chair or counter if you need to. When this exercise becomes less painful, try lowering on one leg only. Repeat 10 times. Do 3 sets of 10. Side-lying leg lift, Lying on your side, tighten the front thigh muscles on your top leg and lift that leg 8 to 10 inches away from the other leg. Keep the leg straight. Do 3 sets of 10.